
From the 1Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Hasanuddin University, Makassar, 2Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Makassar, 3Department of Clinical Nutrition, Faculty of Medicine, Hasanuddin University, Makassar, 4Rheumatology Divison, Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, 5Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Airlangga University, Surabaya, 6Department of Physiology, Faculty of Medicine, Hasanuddin University, Makassar, 7Department of Microbiology, Faculty of Medicine, Hasanuddin University, Makassar, 8Department of Orthopedic, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia, and 9Department of Public Health, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Objective: To assess the effects of dextrose prolotherapy in patients with knee osteoarthritis on the levels of serum cartilage oligomeric proteinase and urinary C-terminal telopeptide of type II collagen, and on the Western Ontario McMaster Universities Index and numerical rating scale score for pain.
Methods: A randomized controlled trial, in which participants were randomly allocated into 2 groups, receiving injections of either hyaluronic acid or dextrose prolotherapy. The hyaluronic acid group received 5 injections, 1 each on weeks 1, 2, 3, 4 and 5, and the dextrose prolotherapy group received 3 injections, 1 each on weeks 1, 5 and 9. Serum cartilage oligomeric proteinase, urinary C-terminal telopeptide of type II collagen, Western Ontario McMaster Universities Index score, and numerical rating scale score for pain were measured at baseline and 3 weeks after the last injection. Comparative analysis was conducted using Wilcoxon test within groups and analysis of covariance (ANCOVA) test between groups.
Results: A total of 47 participants (21 allocated to hyaluronic acid, 26 allocated to dextrose prolotherapy) completed the protocol. Both interventions resulted in significant improvements in numerical rating scale scores for pain, total Western Ontario McMaster Universities Index scores, and its subscales score. However, the dextrose prolotherapy outperformed hyaluronic acid in numerical rating scale score for pain and level of urinary C-terminal telopeptide of type II collagen, with score changes differences of 0.93 (p = 0.042) and 0.34 (p = 0.048), respectively. No significant changes in level of serum cartilage oligomeric proteinase were found in either group.
Conclusion: Dextrose prolotherapy is an alternative injection therapy for knee osteoarthritis, which was found to be associated with a significant reduction in urinary C-terminal telopeptide of type II collagen compared with hyaluronic acid injection. Neither injection method resulted in reduced serum cartilage oligomeric proteinase.
Key words: knee osteoarthritis; prolotherapy; hyaluronic acid; COMP; uCTX-II; functional outcome.
Accepted Apr 8, 2021; Epub ahead of print Apr 21, 2021
J Rehabil Med 2021; 53: jrm00196
Correspondence address: Yose Waluyo, Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia. E-mail: yose.waluyo@med.unhas.ac.id
Doi: 10.2340/16501977-2835
Knee osteoarthritis is a common musculoskeletal disorder, which is one of the most frequent causes of disability in elderly people. To improve patients’ quality of life, prolotherapy has been developed as a non-operative treatment option for osteoarthritis. This study compared the effectiveness of dextrose prolotherapy with that of standard therapy using hyaluronic acid injections. Both interventions were effective in terms of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score improvement and numerical rating scale score changes. Cartilage repair was assessed by measuring levels of specific biomarkers of cartilage breakdown: urinary C-terminal telopeptide of type II collagen (uCTX-II) and serum cartilage oligomeric matrix protein (sCOMP). Dextrose prolotherapy was more effective than hyaluronic acid in reducing these biomarkers and decreasing patients’ pain. Dextrose prolotherapy is therefore recommended for use in patients with knee osteoarthritis, since it gives better results, is cost beneficial, and is suitable for use in low-resource settings. Dextrose prolotherapy may help to repair cartilage in knee OA, as it reduces the uCTX-II level.
Osteoarthritis (OA) is a highly prevalent musculoskeletal disorder, which is one of the most common causes of disability in elderly people (1–3). Several studies have demonstrated the effectiveness of hyaluronic acid (HA) injections, and recent guidelines have recommended their use in knee OA (4, 5). Xin has shown that intra-articular injection of HA (Adant®, Meiji Seika Pharma Co., Ltd., Tokyo, Japan. Manufactured by microbial fermentation and Artz®, Dispo: Seikagaku Corporation, Tokyo, Japan. Manufactured by the extraction of cockscomb), can significantly reduce both the visual analogue scale (VAS) score for pain and the Lequesne index (6). In contrast to these findings, however, a meta-analysis concluded that treatment of knee OA with HA injection did not result in a significantly different outcome from intra-articular placebo, despite the higher costs compared with other common non-operative intra-articular modalities (7).
Regenerative therapy is an alternative approach that has been considered for OA, due to its potential to aid tissue regeneration, improve clinical manifestations, and repair damaged tissue structure, which is the underlying pathological condition in OA (8). An example of a currently developing regenerative approach is prolotherapy, an injection-based modality for treating chronic musculoskeletal pain through the use of substances such as dextrose, phenol-glycerine-glucose (P2G), or sodium morrhuate (9). Previous reports have demonstrated the effectivity of prolotherapy in significantly reducing the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score relative to saline injections and at-home exercise over 18 weeks after injection (10–12). In line with these findings, other reports have shown the promising effects of prolotherapy for tissue regeneration through radiological and arthroscopy-based assessments of cartilage repair (13).
Cartilage oligomeric matrix protein (COMP) and urinary C-terminal telopeptide of type II collagen (uCTX-II) are specific biomarkers used to evaluate cartilage breakdown in OA. Increased levels of these biomarkers can indicate the severity and prognosis of OA (14). Meanwhile, decrease in levels of both biomarkers has been assumed which indicates the improvement in cartilage (15). COMP and uCTX-II are recommended as promising specific biomarkers in OA cases based on Burden of disease, Investigative, prognostic, efficacy of intervention, and diagnostic (BIPED) criteria, as stated in a systematic review (16).
Although previous reports have demonstrated promising potential of HA-based therapy and dextrose prolotherapy (DPT) in improving functional outcome in knee OA, none have compared the efficacy of those modalities in cartilage repair by assessing specific biomarkers, such as serum COMP (sCOMP) and uCTX-II. Hence, the aim of this study was to compare the effects of intra-articular HA and DPT on cartilage repair in knee OA, by measuring the changes in sCOMP and uCTX-II biomarkers.
Study design
The study is a double-blinded randomized controlled trial comparing the effects of DPT vs HA on levels of sCOMP and uCTX-II. Ethics approval was obtained from the Hasanuddin University Ethical Commission (protocol number UH19100814). The study was retrospectively registered on ClinicalTrials.gov (registration number NCT04557943). Primary data collection was conducted from September 2019 to April 2020 in the outpatient unit of the Cerebellum Clinic, Makassar, Indonesia.
Eligibility
Participant eligibility was screened by a trained research assistant, under the supervision of the principal investigator, based on pre-determined criteria. Inclusion criteria were: patients aged > 40 years; and diagnosis of knee OA based on the American College of Rheumatology (ACR) 2012 criteria and radiological examination. Exclusion criteria were: previous intra-articular injection within 3 months; previous use of non-steroidal anti-inflammatory drugs (NSAIDs) one week before intervention; or contraindications to prolotherapy, such as abscess, cellulitis, or septic arthritis.
Recruitment and consent
After confirming the eligibility of the participants, the principal investigator provided a detailed explanation of the study objectives, procedures, the potential effects of the procedure and answered all candidates’ questions regarding the study. Following the explanation, only participants who consented proceeded to baseline data collection.
Baseline measurement
Demographic data, such as age, sex, and body mass index (BMI), were collected. History of illness, previous treatments, baseline numerical rating scale (NRS) for pain and WOMAC scores were also collected. Participants reported their pain intensity score verbally, ranging from 0 “no pain” to 10 “the worst pain imaginable” on the NRS. The WOMAC score was obtained by a trained research assistant: participants were verbally asked about the severity of their osteoarthritis, using the pain, stiffness, and function subscales. The WOMAC composite score was determined, constructed as the total of the 3 subscale scores, range 0 (no limitation) to 96 (worst disability). The severity of KOA was determined by a radiologist using the Kellgren-Lawrence (KL) grading criteria.
Baseline sCOMP and uCTX-II levels were evaluated using an enzyme-linked immunoassay (ELISA) procedure. To assess sCOMP level, 5 ml venous blood was collected and centrifuged at 3,000 rpm for 20 min. The harvested serum was used for COMP measurement using the Human COMP ELISA kit (Bioassay Technology Laboratory, Shanghai, China, catalogue number E1486Hu). To measure uCTX-II level, random urine was collected and centrifuged at 3,000 rpm for 20 min, then the harvested supernatant was used for uCTX-II measurement with the Human CTX-II ELISA kit (Bioassay Technology Laboratory, Shanghai, China, catalogue number E3701Hu). All biomarker assessments were performed at the Hasanuddin University Medical Research Center (HUMRC) Laboratory, Makassar, Indonesia.
Randomization
Simple randomization was used to allocate patients to the 2 groups. A sealed envelope containing the randomized sequence was given to the investigator and care provider, and participants were recruited consecutively. Participants were blinded to the therapy by receiving individual treatment in different rooms and on different occasions. On the day of assessment, the physician and laboratory technicians were blinded to group allocation.
All data collections were performed by trained research assistants who were blinded to the patients’ allocation status via face-to-face interviews. External personnel were employed to perform data entry, so that the statistician could analyse data without referring to the allocation information, thus ensuring blinding. The envelope was opened at the end of data analysis.
Interventions
The interventions were performed by the principal investigator (a trained physician). The HA group was given a 2 ml Adant® intra-articular injection (~10 mg) on weeks 1, 2, 3, 4 and 5. The DPT group was given a 5 ml 25% intra-articular dextrose injection and 30–40 ml 15% peri-articular dextrose injection in several sites, such as the medial collateral ligament, pes anserine, tibial tubercle, coronary ligament, patellar edge, lateral collateral ligament, and tibiofibular ligament. DPT injections were administered on weeks 1, 5 and 9. Participants were advised to take only acetaminophen (500 mg every 8 h, as needed) if the pain flared up and to avoid NSAIDs in the first 72 h after injection. Participants were contacted every day for one week after the injection to assess side-effects.
Outcomes
sCOMP and uCTX-II measurement. The primary outcomes of this study were changes in sCOMP and uCTX-II as specific biomarkers of cartilage degradation. Both the sCOMP and uCTX-II levels were obtained at baseline and 3 weeks after the final injection, using the ELISA methods described above.
NRS and WOMAC scores. The secondary outcomes of this study were changes in pain scale, assessed by the NRS score, and functional outcome, assessed by the WOMAC score. NRS score was obtained at baseline and 3 weeks after the final injection.
Statistical analysis
Sample size calculation. Based on a previous study using WOMAC score as the outcome variable after DPT intervention (12), the sample size was calculated using σ2 = 0.09 and (μ1–μ2) value = 0.05 (12), Z1-α/2 value = 1.96 with 95% confidence interval (95% CI) and Z1–β value = 1.282 with 90% power. The possibility of participants dropping out was anticipated, hence the minimum total sample for this study was 18 in each group.
Analysis. Per-protocol analyses were performed for the data of participants who completed all the study protocols. The pre- and post-intervention NRS scores, WOMAC and its subscale score, sCOMP level, and uCTX-II level were analysed in both groups using the Shapiro–Wilk test to interpret data distribution. Subsequently, comparison of pre- and post-intervention NRS scores, WOMAC score, sCOMP level, and uCTX-II level in both groups were analysed using the Wilcoxon test. At baseline, there were differences between the DPT and HA groups in terms of NRS score, pain WOMAC score, functional WOMAC score, and total WOMAC score. Therefore, one-way analysis of covariance (ANCOVA) was used to compare between 2 groups, using the baseline value of NRS, pain WOMAC, functional WOMAC, and total WOMAC as covariates. A p-value < 0.05 was considered significant. Statistical Package for the Social Science (SPSS) version 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, New York: IBM Corp) was used for all analyses.
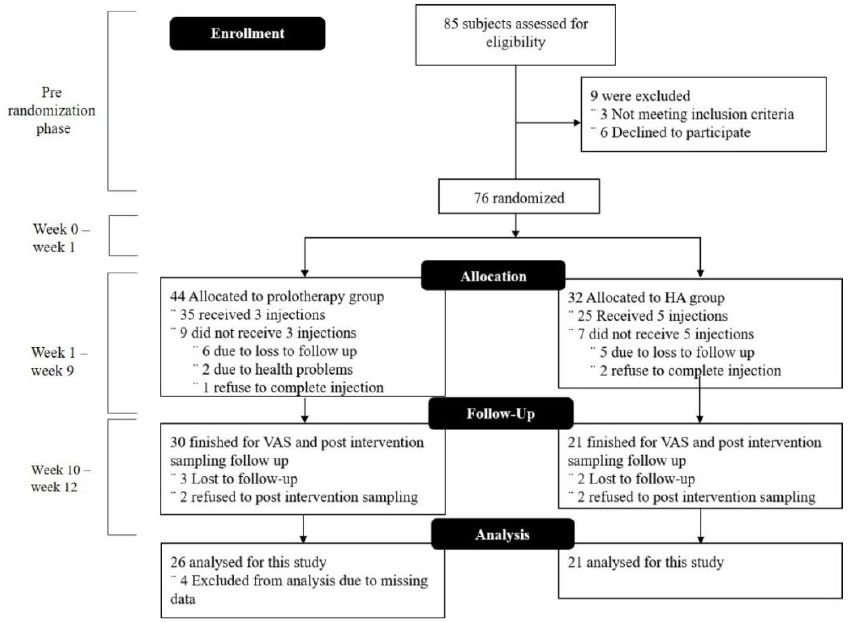
As shown in the flow chart (Fig. 1), 85 participants were enrolled in the first screening. Of these, 3 participants were excluded as they did not meet the inclusion criteria, and 6 were excluded after refusing the injection. A final total of 76 participants were included in the study, of whom 44 were allocated to the DPT group and 32 to the HA group (some participants in HA group did not receive the intervention because they declined the intervention after randomization). Among the participants receiving DPT, 35 received 3 injections, and only 30 completed the follow-up. In the HA group, 25 participants received 5 injections, and only 21 completed the follow-up. Hence, at the end of the study, the number of participants included for analysis were 26 from the DPT group and 21 from the HA group. The trial recruitment stopped once the minimum sample size for the study was fulfilled.
Fig. 1. Participants’ flow chart. VAS: visual analogue scale; HA: hyaluronic acid.
Due to the high level of drop-out of participants, baseline data for per-protocol subjects and excluded subjects were compared in order to determine potential biases. There were no significant differences between per-protocol subjects and subjects excluded in both groups.
The 47 participants included for analysis were mostly female (74.5%) and obese (53%), with an mean age of 62.4 years (standard deviation (SD) 8.7) (Table I). Before intervention, the mean NRS score of the DPT group was 4.85 (SD 1.71), and that of the HA group 3.48 (SD 1.53). The mean WOMAC total score and its subscales (pain, stiffness, and function) for the DPT group were 36.08 (SD 10.06), 7.15 (SD 3.09), 3.08 (SD 2.24), and 25.85 (SD 7.88), respectively; and for HA group 24.81 (SD 17.25), 4.90 (SD 2.93), 2.52 (SD 1.83), and 17.38 (SD 15.99), respectively. Baseline uCTX-II and COMP levels in the DPT and HA groups were 1.19 ng/ml (SD 0.41 vs 1.01 ng/ml (SD 0.39) and 1,240.5 pg/ml (SD 2,161.1) vs 1,917.1 pg/ml (SD 2,821.5), respectively. A complete profile of the participants and the baseline measurement of studied parameters are shown in Table I.
Table I. Characteristics of participants and baseline measurement of parameters
A complete course of DPT injections was given to 26 of the 47 participants (pre- and post-intervention scores are shown in Table II). Participants showed significant improvement in NRS score, WOMAC total score, and all subscale scores of WOMAC. Assessment of biomarkers revealed a significant reduction in uCTX-II level (0.25 ng/ml; p = 0.032), and a slight reduction in sCOMP level (p = 0.137). Meanwhile, the 21 participants who were given HA injections showed a significant decrease in NRS score (1.61; p = 0.002). The total and subscale scores of WOMAC also decreased significantly (Table II). Both uCTX-II and sCOMP levels increased, but showed no significant changes, with score changes of 0.05 ng/ml (p-value = 0.404) and 810.7 pg/ml (p-value = 0.274), respectively.
Changes in NRS score, WOMAC score, uCTX-II level, and sCOMP level for both groups were compared by adjusting the data. A significant difference was demonstrated in the NRS score and uCTX-II level between the DPT group and the HA group, with score changes of 0.93 ng/ml (p = 0.042) and 0.34 ng/ml (p = 0.048), respectively (Table II).
All participants experienced expected mild-to-moderate post-injection pain within 2–3 days. Only one participant, from the prolotherapy group, took paracetamol due to a painful knee post-injection. There were no other side-effects or adverse events.
Table II. Baseline and score changes in numerical rating scale for pain, Western Ontario McMaster Universities Index (WOMAC) score, and specific biomarker in both groups
Knee OA is a common musculoskeletal disorder in old age. Participants in this study were mostly elderly, obese and female. These characteristics of the participants are known as the risk factors of knee OA based on previous study (17). Prolotherapy is a non-operative treatment, which has been developed to improve quality of life in patients with osteoarthritis. Prolotherapy is an injection-based treatment that is commonly used in chronic musculoskeletal pain conditions. Although it has been identified as regenerative therapy (18), it differs from other regenerative injection therapies, such as platelet-rich plasma (PRP) and stem cell injection, by the absence of a biologic agent. The current study compared the effectiveness of injection therapies with DPT and HA, by assessing specific biomarkers as the primary outcome in addition to several functional outcomes. Although both groups showed significant improvement in NRS and WOMAC scores, only the DPT group showed a significant decrease in uCTX-II level. In contrast, previous studies showed either an increase (19) or decrease (20) in uCTX-II level following HA intervention.
The uCTX-II level is one of several cartilage degradation biomarkers, wherein increased levels of uCTX-II correlate with radiological severity and cartilage thinning on magnetic resonance imaging (MRI) examination (14, 21, 22). And while the chondrogenic effects of prolotherapy remain unclear, several in vitro studies have shown that human cells produce various growth factors after exposure to hypertonic dextrose (23). Hypertonic dextrose solutions act by dehydrating cells at the injection site, leading to local tissue trauma, which, in turn, attracts granulocytes and macrophages and promotes healing. Other studies stipulate that the injected proliferant imitates the natural healing process of the body through initiation of a local inflammatory cascade, which triggers the release of growth factors and collagen deposition (24, 25). In addition, a low-level chondrogenic effect of dextrose has been demonstrated by Topol et al. (13), through observation using arthroscopy. It is therefore assumed that this chondrogenic effect of dextrose on cartilage may be reflected by a decreased level of uCTX-II.
In this study, no significant change was observed in sCOMP level in either interventional group. To our knowledge, no previous studies have observed the effect of these 2 interventions on sCOMP levels. In OA, COMP correlates with non-collagenous protein in cartilage (14) and is a promising biomarker of cartilage damage, which can be used for early detection and assessment of disease progression (26, 27). However, COMP elevation is not specific to knee OA; some studies have shown that sCOMP level can increase in joint trauma or excessive physical activity (28, 29). In addition, increased sCOMP level is also found in malignancies of the breast, prostate, and colon (30, 31). Since the current study did not exclude patients who had disease history or comorbidities, these may have affected sCOMP levels in this study.
Both interventions showed favourable changes in the secondary outcome of WOMAC total score and NRS score. However, the NRS score changes were more remarkable using DPT intervention. The favourable changes in pain score and functional outcome in HA and DPT shown in this study are in line with the results of previous studies (11, 12, 32–35). As described previously, DPT outperformed HA in improvement of pain score. However, the mechanism of pain reduction of these agents is not fully understood. Previous studies have indicated that HA may reduce pain through anti-inflammatory mechanisms by binding to the cluster of differentiation 44 (CD44) receptors. This leads to inhibition of IL-1β expression by inducing mitogen-activated protein kinase phosphatase (MKP)-1, eventually decreasing the production of catabolic enzymes (MMP 1, 2, 3, 9, and 13) that has been known to induce inflammation in the synovium (36, 37). Meanwhile, the pain reduction mechanism in prolotherapy is assumed to occur by its capacity to promote growth-factor mediated tissue healing (38, 39), provide desirable nutrients necessary for regeneration (38), exert a potential direct effect on peripheral nerves (39), and strengthen the ligament and tendons, which have been considered as the source of pain in KOA (35, 41). Those mechanisms may be associated with cartilage and peri-articular structure repair, which eventually leads to reduction in pain and improved joint function. Although there was no significant change in WOMAC scores between groups, the mean improvement on WOMAC score in the DPT group was 16.92 points (SD 13.85) , which exceeded the minimal clinically important difference (MCID) on the WOMAC for knee OA, which is 12 points (12). Meanwhile, the mean WOMAC score change in the HA group was 8.95 points (SD 9.79), which is not close to a significant clinical change. This fact might indicate that the current study is underpowered; larger studies are therefore needed to evaluate the effect more comprehensible.
Study limitations
Although this study is the first to report the alteration in cartilage biomarkers after DPT and HA intervention in knee OA, some limitations should be noted. The study is substantially limited by the level of dropout, which introduces considerable bias regarding the magnitude of positive outcomes. It is also substantially limited by the between-group difference, although these were corrected by covariate analysis. Previous disease or comorbidities of participants may have confounded the biomarker levels in this study. The small sample size and homogenous ethnicity of the participants also restrict the generalizability of this study; hence, future studies should examine a larger, more comprehensible, and more representative subject population.
Conclusion
DPT is a promising alternative injection therapy for KOA, which resulted in more favourable changes in uCTX-II level relative to HA injection therapy. Both injection therapies demonstrated good functional outcome and pain reduction.
The authors thank the Dean and Vice Deans of the Faculty of Medicine Hasanuddin University, the Physical Medicine and Rehabilitation Department, and the Cerebellum Clinic for their support. Great appreciation is also given to Gita Vita Soraya, Ahmad Yasin, Sari Rajwani Artika, and Insani Nanda Wahyuni for their assistance while conducting this study.
Ethics approval. The study was approved by the Faculty of Medicine Hasanuddin University Ethics Committee on 12 November 2019 (protocol number UH19100814). The trial (NCT04557943) was registered at ClinicalTrials.gov on 22 September 2020.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize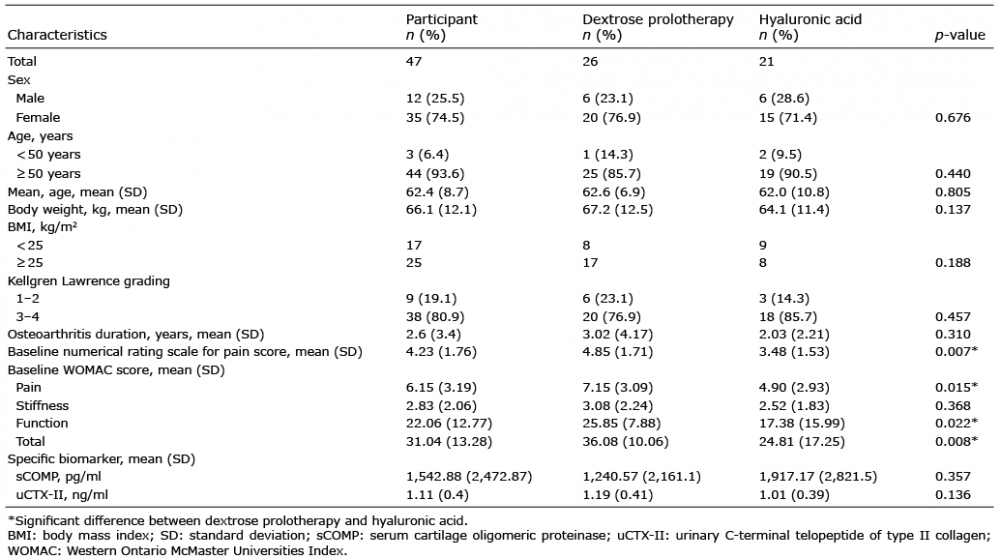 Click to show fullsize
Click to show fullsize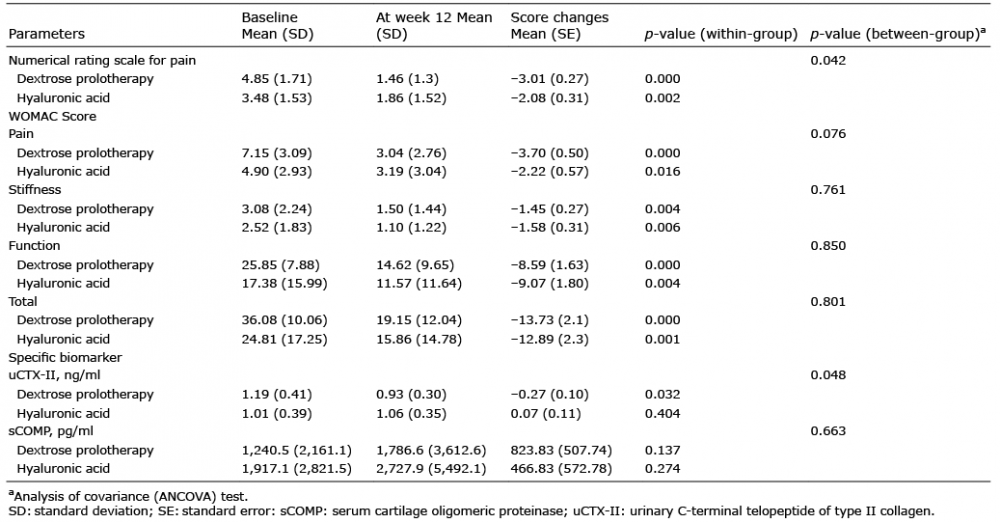 Click to show fullsize
Click to show fullsize